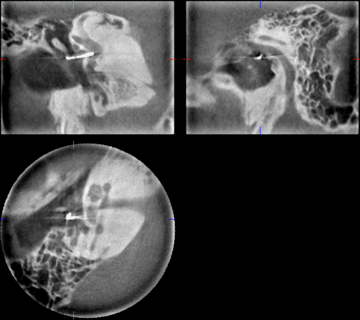
More and more radiology practices are using the added value provided by CBCT as a supplement to CT. The advantages of CBCT are better detailed images because of much smaller voxel sizes, lower slice thickness, minimal artifacts and lower radiation dosage. Radiology combines the areas of indications of ENT, plastic surgery, skull base surgery, ophthalmology, maxillofacial surgery, and dental applications. Due to its ability to capture a variety of image volumes (fields of view or FOV), it can be used in temporal bone diagnosis; providing high definition images of the superior semicircular canal dehiscence, otosclerosis, ossicular chain dislocation, cholesteatoma, as well as images suitable for navigation systems.
-
Our solution.

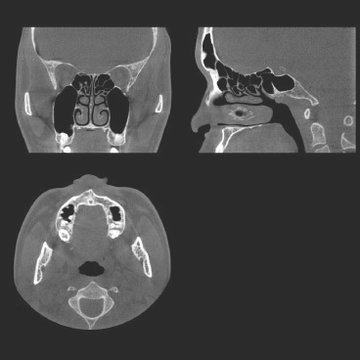
The CBCT scanner, 3D Accuitomo 170, is an ideal imaging system for your radiology practice. It provides detailed views of very fine anatomical structures in the areas of the head and neck, such as the temporal bone, paranasal sinus, eye sockets, jaw and skull base. Consequently, it can be used for ENT, plastic surgery and all dental indications.
-
Benefits of the technology
Safe diagnosis
Three-dimensional imaging has one significant advantage: it can visualize anatomical structures in high definition. Hence, the doctor can obtain more data from the information because the true location of anatomical structures can only be discerned with a three-dimensional visualization. Accordingly, it helps make for safer diagnoses.
Reduction of radiation dosage
Patients also benefit from a CBCT scan because the radiation dosage is significantly lower than that of a conventional CT. In the latter case, the radiation source scans the region of the body that is to be examined in slices of 0.5 to 3.0mm; CBCT scans the entire section in one single rotation. As a result, the dosage is reduced by up to 80 percent as compared to a standard CT X-ray*.
* 1mm slice thickness, 1.5mm pitch, 120 mAS/rotation, 87mm scan height
-
Technology

Spatial orientation based on cone-shaped X-ray beam
CBCT works on the basis of a cone-/pyramidal-shaped X-ray beam: for this purpose, a flat panel detector and an X-ray source are mounted on opposite sides of a rotating arm. The physician positions the patient in the isocenter, and the C-arm rotates at least 180° during the scanning process. While the scanner is rotating around the patient, the projection of a cylindrical volume is obtained at defined view angles with the cone-shaped X-ray beam.
-
Indications
Rhinology
- Sinusitis
- Paranasal cavity
- Image acquisition of IGS for FESS
- Orbital blowout fracture
Otology
- Cholesteatoma
- Otosclerosis
- Mastoiditis
- Ossicular chain form
- Cochlear implant (CI)
- Semicircular canal dehiscence syndrome
- Congenital abnormalities of the middle ear
- Patulous Eustachian tube (PET)
- Temporal bone fracture
Laryngology
- Diagnosis of foreign body larynx (in the case of X-ray opaque)
- Ptyalolith (in the case of X-ray opaque)
Skull Base Surgery
- Endoscopic transnasal approach for skull base surgery with image guidance system
Plastic surgery
- Cleft palate
- Trauma of the maxillofacial area
- Orbital blowout fracture
- Zygomatic arch fracture
- Nasal fracture
Ophthalmology
- Nasolacrimal duct obstruction
Dental
Periodontology
- Visualization of the marginal bone contour
- Three-dimensional visualization of intrabony pockets and furcation defects
Endodontics
- Visualization of the marginal bone contour
Orthodontics
- Formation of the roots
- Location of teeth and tooth germs
- Resorption
- Obstacles to movement
- Presence of periodontal space
Dental surgery
- Retained, dislocated teeth (wisdom teeth, canines, premolars, surplus teeth and/or dental germs)
- Apical periodontitis, radicular cysts
- Pre- and post-operative visualization of important anatomical structures (course of N. alveolaris inferior , mental foramen, floor of the nose, osseous sinus restriction) for dental-surgical procedures, fractures
- Implant planning and control
- Patients with lip-palate-jaw clefts (depiction of the bone structure in the region of the cleft jaw)
- Temporomandibular joint diagnostics



